Definition of “First Aid” = First assistance rendered to a patient in any injury/illness emergency situation.
Definition of “Duty to Act” = No rescuer is ever required to render aid, based solely upon the fact that he/she is trained to do so. However, workplace expectations may state that a student is required to assist, as part of his job duties, in an emergency situation.
Persons choosing to assist a patient are protected in most States from successful prosecution by “Good Samaritan Laws”. These laws state that if the rescuer: “Does what he/she has been trained to do”, “to the best of his/her ability”, “in the best interest of the patient” and “does not receive compensation for his/her assistance” that person may not generally be successfully prosecuted for issues arising from that assistance. (Note: Healthcare Providers rendering aid while performing their jobs are typically covered by their employer’s liability insurance.)
1) If considering treatment of an adult, tell the patient you are able to assist and request permission to do so. A competent adult may refuse assistance – in which case the rescuer may call 911 and request assistance from EMS providers. (An adult would not be considered competent while exhibiting “altered mental status”, in which case the rescuer should call 911 and describe the situation.) When considering treatment of a minor, attempt to obtain permission from immediately available parents/guardians. If no one is with the minor, assume you have consent to treat him.
2) To determine whether assistance is necessary, rescuers should attempt to “find the problem”. If the patient is conscious, ask the patient.
If the patient is not conscious, or cannot respond, ask bystanders or family members for information and follow these steps:
A) Determine scene safety.
B) Determine the level of the patient’s response.
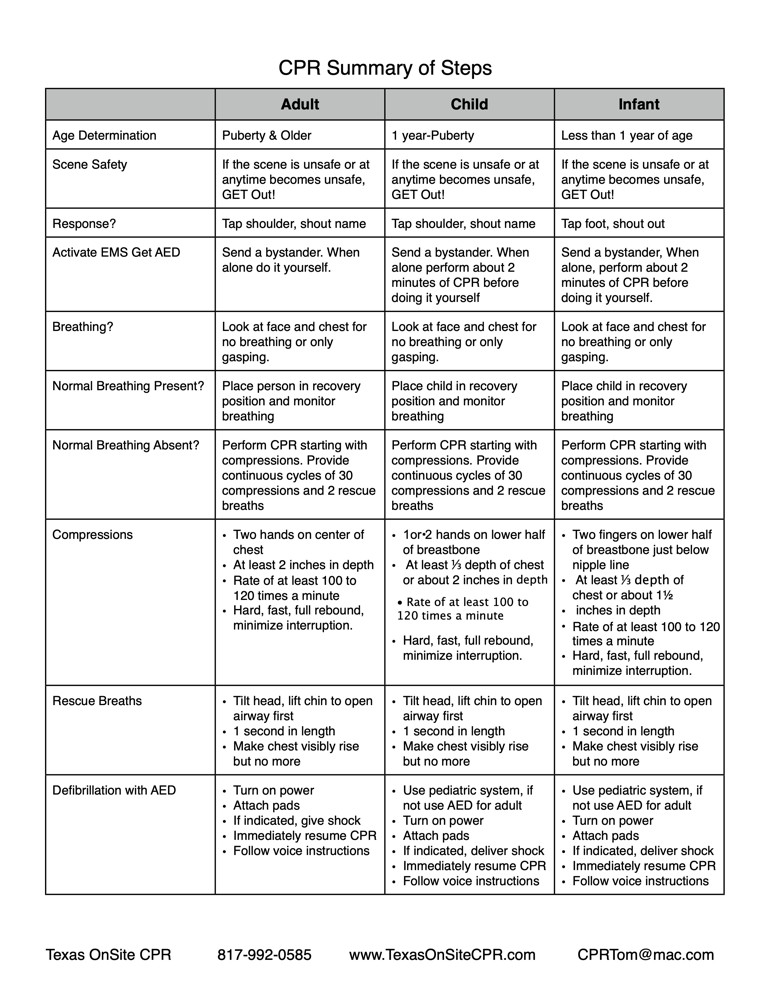
C) Is the patient breathing normally?
D) If yes, should 911 be called?
E) If no, call 911 and get an AED.
F) Check for and correct immediate life threats. (Control profuse bleeding; begin CPR.)
G) If no immediate life threats. treat secondary issues. Look for medic alert jewelry; get bystander information.
3) Most pediatric fatalities are the result of accidents and/or injuries. Prevention is crucial!! Quick treatment is also critical because children often show few symptoms for serious issues until they become life-threatening.
All children should ride in approved automobile child restraints, including booster seats, until they are at least 8 years old, weigh 65 pounds or are a minimum of 4’ 9” tall. If the child can sit on the car seat with his back touching the back of the seat and his knees bend at the edge of the car seat (it is not necessary for his feet to touch the car floor) then he can safely be restrained in the vehicle’s lap/shoulder belt. (Serious internal injuries can occur if a child whose knees do not bend at the edge of the car seat is restrained solely in a lap/shoulder belt system.)
When rendering First Aid, the best way to prevent potential contamination is to wash your hands frequently and wear gloves and other personal protective equipment. To be effective at preventing contamination, gloves should not only be worn but should also be removed properly. Improper glove removal can lead to inadvertent contamination. Always put on gloves before beginning treatment. Wash the wounded area with soap and running water if possible, to clean the area and determine the scope of the injury.
To safely remove gloves:
1. Grasp the palm of one glove between the thumb and forefinger of the other gloved hand. Pull that glove straight off over the fingers, pulling the hand out of the glove. Keep the removed glove in the still-gloved hand.
2. Completely envelop the removed glove in the gloved hand so no parts of it are hanging loose to contribute to potential contamination.
3. Put two fingers under the cuff of the back side of the remaining glove.
4. Pull that glove off the hand, over the closed fist, being careful not to touch any outside parts of the glove or the cuff of the glove.
5. Grasp the removed gloves only near the fingers, not near the cuff, and dispose of properly.
6. Used gloves may be disposed of in a biohazard bag or a Ziploc type bag which can be sealed; or they may be sealed into a plastic “grocery type” bag which is then sealed into another “grocery type” bag for disposal with standard trash.
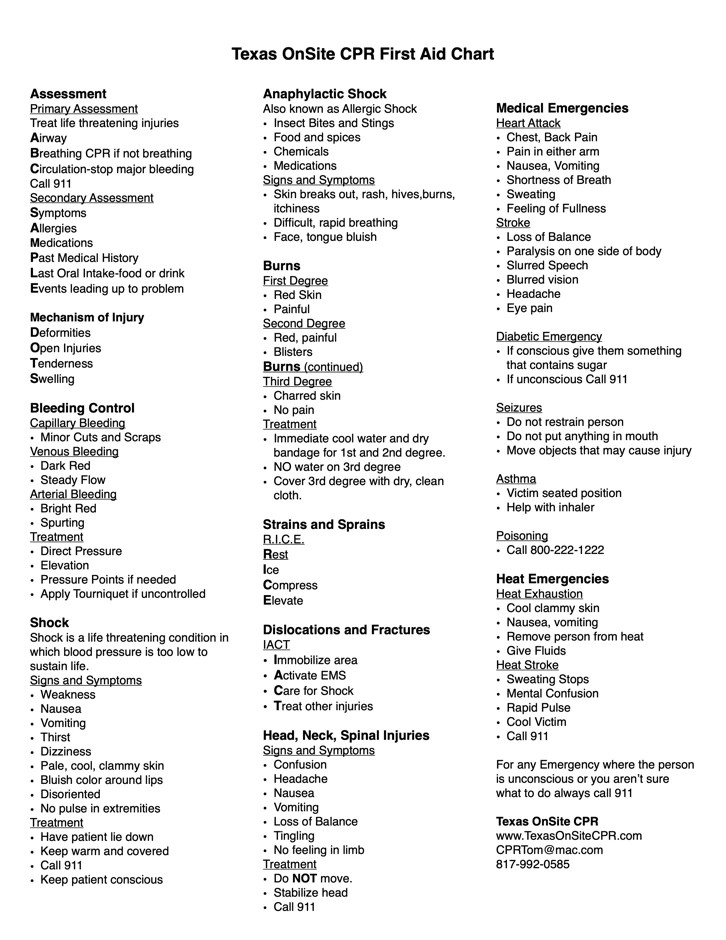
MEDICAL EMERGENCIES
HEART ATTACK – Symptoms:
- Chest pain – dull, crushing, burning
- Back pain – upper or lower
- Pain in either arm
- Pain that radiates from one area to another – ie. back or chest to neck and/or jaw
- Nausea
- Vomiting
- Shortness of breath or trouble breathing
- Cold, clammy sweat
- Feeling of fullness or indigestion
- Mental distraction or “disconnect”
- Increased foot or hand pain (diabetics)
- Denial
- Always call 911 for any suspected heart attack – time is critical!
- Have the patient sit comfortably or lie down and rest.
- Ask the patient to cough forcefully at regular intervals.
- If the patient is conscious and can swallow, have him/her chew and swallow one non-coated 325 mg aspirin tablet (or two to four 81 mg “baby aspirin”).
- Be prepared to start the steps of CPR and use an AED.
STROKE – Symptoms:
- Loss of balance
- Paralysis or loss of muscle control on one side of the body
- Facial droop
- Slurred, unintelligible or inappropriate speech
- Altered mental status
- Sudden severe headache with no known cause
- Blurred vision
- Eye pain
- Always call 911 for a suspected stroke! Treatments must begin within 3 hours of the first onset of symptoms.
- Never administer aspirin if a stroke is suspected.
- Be prepared to start the steps of CPR and use an AED.
DIABETIC EMERGENCY – Symptoms:
- Altered mental status – patient acting confused, combative, dazed, excessively tired
- Loss of consciousness
- Excessive thirst
- Excessive urination
- “Fruity” or “alcohol” smelling breath
- Seizures
Diabetic emergencies indicate low blood sugar and can be life threatening!
If the patient is conscious and can swallow, give him/her something with sugar to drink and/or eat – fruit juice, soda (not diet), sugar or honey packet, cake icing, candy.
1 Call 911 if the patient loses consciousness or does not respond well to sugar.
SEIZURE
A seizure is a symptom of another problem. Seizures can be a result of: fever, head injury, infection, seizure disorders (ie. Epilepsy), heat stroke, stroke, poisoning and low blood sugar.
- Call 911! Do not restrain anyone seizing.
- Do not put anything in the person’s mouth.
- Move objects away from the person so they do not injure themselves.
- Allow time for the person to recover normal physical and mental capabilities.
- If the seizure lasts for more than 5 minutes or there are more than 5 seizures sequentially, be prepared to begin CPR.
ASTHMA
Asthma attacks can be triggered by: extreme temperatures (hot/cold), exertion, allergies and stress.
- Seat the person comfortably upright, away from the attack trigger if possible.
- If trained, assist the person with his/her prescribed inhaler.
- Call 911 if the person continues to have trouble breathing!
CHOKING
Choking is a fairly common occurrence in both children and adults. You might suspect an adult or child is choking if the person:
- Cannot speak
- Cannot cough loudly
- Makes the choking sign (holds his neck with one or both hands)
- Has bluish lips or skin
If you suspect the person is choking ask, “Are you choking?” If the person speaks, ask him to cough loudly. If the person nods, “Yes”, tell him you can help him; if he’s an adult, ask his permission to help. “I can help you, is it OK if I help?”